 |
| Sunrise last week; sunset this week. |
Before I mumble on with more tales from Holy Cross, could I urge you to click on the following link and sign the “ePetition,” asking the Eastern Cape Department of Health to get organised. We have already lost one potential doctor as a result and there are other hospitals facing a very real prospect of being “doctor-less” by August – the implications of this are massive.
***
If you stumbled into casualty on Sunday evening you may have wondered why I was standing on top of an 80 year old patient’s bed with my leg in his armpit and pulling the man’s arm with all my might (may I add that my raw strength is probably equivalent to that of a five year old). Firstly, I do not believe for one second that he was 80. However, he was definitely pushing it and was built like the Terminator. This could be a slightly histrionic statement, but that’s how it felt. Years of working the land had made this elderly gentleman rather “ripped.” I guess you may be asking why I was pulling back on his arm, with a nursing colleague giving counter traction via a bed sheet strapped around his armpit. The old geeza had rather impressively dislocated his shoulder. Now, I have done this on two occasions myself (one skiing and one throwing some slightly over enthusiastic shapes on the dance floor) – it is exceptionally painful. Fortunately for myself, as mentioned earlier, I sometimes look a little malnourished (hence, a lack of muscle bulk) and I had my doctor friend George (we were medical students at the time) to slip it back in – I am and always will be eternally grateful for this. Hence, I could almost understand how the old fella was feeling.
In general there are three ways to dislocate a shoulder – either it comes forward (the commonest injury and what I had), goes backwards or heads down, into the armpit. He had all the classic signs of a dislocated shoulder: agonising pain, loss of the angle of the shoulder and reluctance to use the arm. However, his arm was also held abducted (i.e. hanging out – he couldn’t bring his arm to his side). A quick examination revealed that he had also sustained a possible nerve injury and that his humeral head (the ball joint at the top of ones humerus – quite self explanatory really) was sitting in his axilla (armpit). So, I gave him a good dose of pain relief and sedation, then tried my best to plonk it back with the assistance of two nurses.
It is only the second dislocation I have seen here, but both have been inferior ones – from what I have read, they are rather rare and can be a bugger to relocate (orthopaedic colleagues, please correct me if I am wrong). The reason I keep mentioning muscle bulk is because the more there is, the harder it is to pull a joint back into position. Fortunately, the first time I saw this it was an elderly lady who’s shoulder was only slightly smaller than mine – I reduced it with no problem at all, except for her responding a bit too enthusiastically to the trickle or morphine that I gave her.
After 45 minutes of pulling, twisting, getting the book out, trying different manoeuvres and pulling again, I accepted defeat. I think this point was realised when I found myself using the bed as a pivot to lean back and almost falling over from my own fatigue. So, I sent him to our orthopaedic hospital with plenty of analgesia in his system – a bumpy 4 hour trip is not ideal at the best of times, let alone with a fracture or dislocation.
***
Assaults are common here; so are guns. Hence, there is a big sign on the hospital front that clearly says: “No guns.” It makes sense, hospitals are places for healing; guns are designed to cause harm. There I was performing an examination on a security guard from a supermarket in town, who had been beaten up by a couple of men. He told me that the men were having an argument in the store, so he tried to break up and settle the dispute, or at least move it outside. Instead of agreeing they gave him a few punches and ran off to fight elsewhere.
The guard was fine, but as I asked him to: “Khulula,” (undress, in Xhosa), I found that he was packing heat. For a little clarity, that is the “gangsta” lingo for carrying a firearm. It just so happened that at this point my nurse had popped out of the consulting room and it was only the two of us. I very kindly told him that yielding a gun in a hospital was completely unacceptable, but decided to leave it at that. I was more concerned that if I alerted the security, the situation could have gone from very pleasant to bang, bang.
***
Medical ward can be hard work, both mentally and physically. However, yesterday I discharged a nice lady who had suffered a stroke. Before I had time to blink, she hobbled up to me (it’s not so easy to run when half of your body doesn’t do what you tell it) and gave me lots of kisses and a showering of: “Siyabonga, siyabonga,” (thank you, thank you). It’s these moments of spontaneity that one just doesn’t get in other lines of work – I wouldn’t change my job for anything.
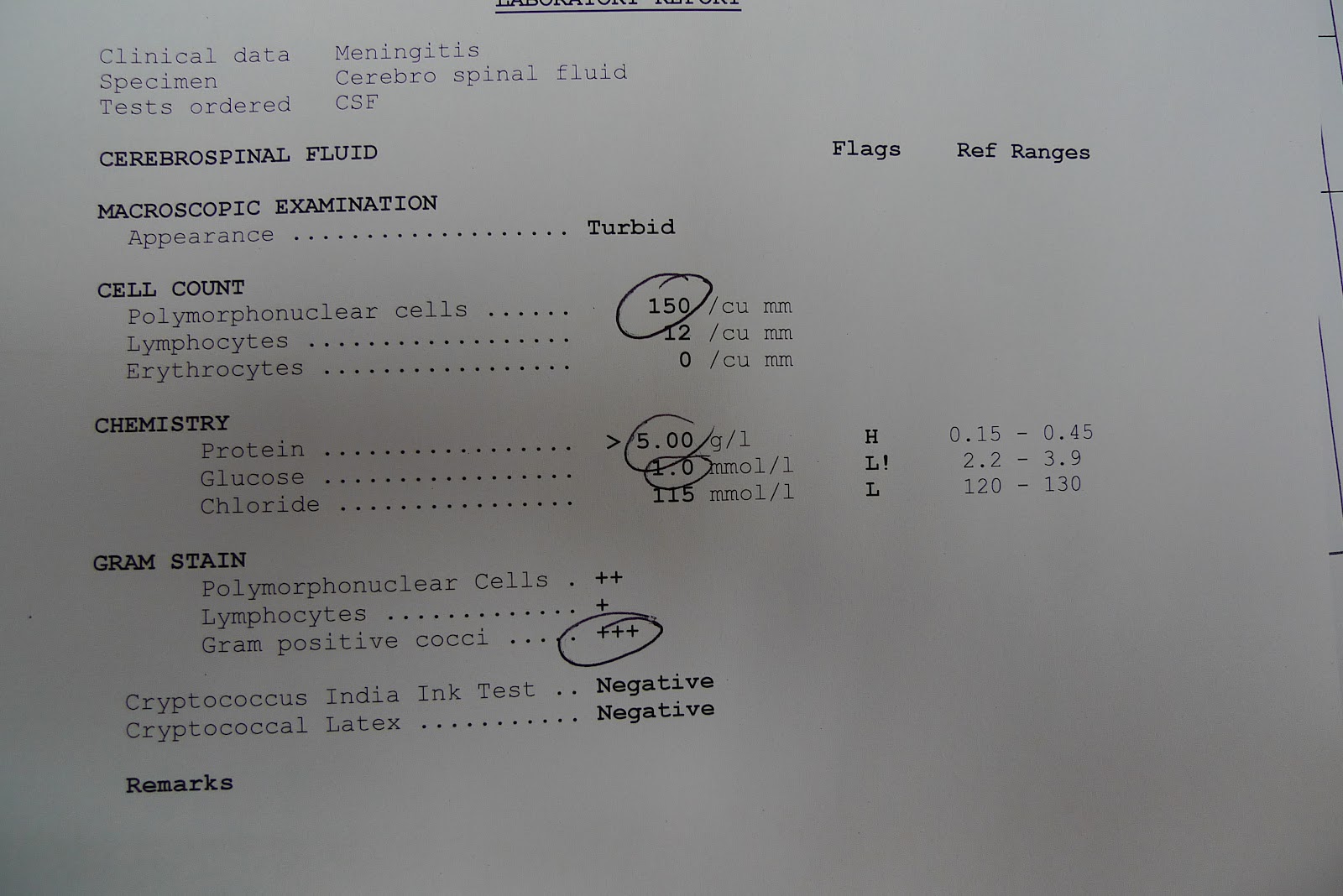 |
| A classic CSF picture of bacterial meningitis. Unfortunately, the young man was dumped onto a bus in Durban back to the Eastern Cape and by the time I saw him he was too far gone. He died later the same day. |
 |
| This is the chest xray of a rather well looking young man who had some persistent TB symptoms. The big blob in the middle is his heart surrounded by a load of fluid (pericardial effusion) that I confirmed on ultrasound. Extrapulmonary TB is the commonest cause of pericardial effusions here. |
 |
| This lady had fallen over the week prior and was hobbling around in excruciating pain. Notice that her left leg is a little shorter than her right and that the left ankle is rotated outwards. This is a typical of a fractured hip. |
 |
| A very jaundiced patient. Notice the reflection of my favourite Sister in medical ward. |
 |
| This is the young mother who had Steven's-Johnson Syndrome - she is on a full road to recovery and I have sent her home to be with her child. She's due to come back for review in two weeks. (Images use with permission of patient) |
 |
| A massive lipoma (fat deposit) that I removed from a lady's arm. An exceptionally satisfying procedure. |

